
Accurate coding for burn injuries is critical in healthcare, requiring a detailed understanding of various factors. As a medical coder, familiarity with burn types, extent estimation, and coding guidelines is essential for precise documentation and billing. Given the high incidence of burn injuries requiring medical attention, mastering burn care CPT coding is a vital skill. This guide will provide an in-depth look at burn classifications, coding methodologies, and practical applications to enhance your coding accuracy and efficiency.
Defining Burn Injuries and Their Classifications
A burn injury is defined as tissue damage resulting from heat, chemicals, electricity, radiation, or sunlight, leading to partial or complete skin destruction. Common causes include scalding from hot liquids, fires, and flammable substances. Inhalation injuries, caused by smoke inhalation, are also classified as burns. It’s important to note that while ICD-10-CM distinguishes between burns and corrosions, the coding guidelines remain consistent for both.
Types of Burns: Understanding the Causative Agents
Burns are categorized based on their source, which influences the nature and extent of the injury:
- Thermal Burns: These are the most common type, resulting from direct contact with heat sources like fire, hot liquids, or steam. The heat causes cell death and tissue charring.
- Electrical Burns: Occurring when the body encounters an electric current, these burns can be deceptively severe. The visible external damage may underestimate the extensive internal tissue and muscle damage.
- Radiation Burns (Radiation Dermatitis): This type of dermatitis is triggered by exposure to radiation from sources like radiation therapy, fluoroscopy, welding arcs, sunlight, and tanning beds.
- Chemical Burns (Corrosions): Caused by contact with corrosive substances such as strong acids (bleach, battery fluid) or alkalis (ammonia, detergents, solvents). These burns can affect both internal and external body parts.
The severity of a burn is determined by its depth and the total body surface area (TBSA) affected. Severe burn injuries often involve areas of varying depths, complicating treatment and increasing the risk of complications like infections and scarring.
Degrees of Burns: Assessing Burn Depth
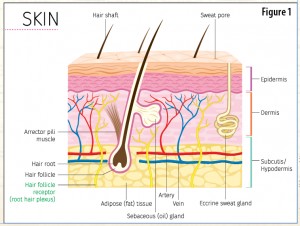
Burn depth is classified into six degrees, each indicating the layers of skin affected (refer to Figure 1 for visual representation of skin layers):
- First-Degree Burns: Superficial burns affecting only the epidermis, the outermost skin layer. Characterized by redness (erythema), pain, and dryness, they typically heal within a week without scarring. Sunburns are a common example.
- Second-Degree Burns: Partial-thickness burns that damage the epidermis and extend into the dermis, the layer beneath. Blistering is a hallmark of these burns. Severe second-degree burns may require skin grafts and can result in scarring.
- Third-Degree Burns: Full-thickness burns causing complete destruction of both the epidermis and dermis, including hair follicles, sweat glands, and oil glands. Skin grafts are always necessary for healing.
- Fourth-Degree Burns: Burns extending beyond the skin into the subcutaneous fat layer.
- Fifth-Degree Burns: Burns reaching the muscle tissue.
- Sixth-Degree Burns: The most severe, extending down to the bone.
Figure 1: Cross-section of skin layers illustrating burn degrees.
When coding for patients with burns in multiple anatomical locations, remember these guidelines:
- Code each burn location separately.
- For multiple burns at the same anatomical site, code only the most severe burn.
- Sequence codes by severity, listing the most severe burn first.
In cases involving both internal and external burns, the reason for admission dictates the principal diagnosis. For instance, if a patient is admitted for burn injuries along with related conditions like smoke inhalation, the burn injury would typically be the primary diagnosis.
ICD-10-CM Burn Coding: Utilizing the Rule of Nines
ICD-10-CM coding for burns requires specifying body location, depth, extent, and external cause. Accurate burn diagnosis coding necessitates at least three codes:
-
First-listed Code(s): Site and Severity (Categories T20-T25)
- The primary code combines the burn site and severity. Categories T20-T28 classify burns by general body region.
- The fourth character denotes burn severity (except for categories T26-T28), using burn degrees.
- The fifth character provides further anatomical site specificity.
- The sixth character indicates laterality (left or right side).
-
Next-listed Code: Extent of Burn (Categories T31/T32)
- Burn extent, or the percentage of TBSA involved, is crucial for coding.
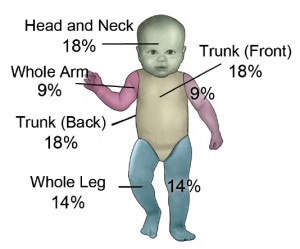
- Codes from T31 (burns) or T32 (corrosion) are used, based on the “Rule of Nines” (see Figure 2).
- The Rule of Nines assigns percentages to body areas: 9% for the head, 9% per arm, 18% per leg, 18% for the anterior trunk, 18% for the posterior trunk, and 1% for the genitalia in adults.
- A modified Rule of Nines is used for infants, accounting for their larger head (18%) and smaller legs (14% each).
- The fourth character in T31/T32 codes represents the total percentage of TBSA affected by burns.
- The fifth character indicates the percentage of TBSA with third-degree burns specifically.
-
Additional Code(s): External Cause Codes (Optional but Recommended)
- ICD-10-CM guidelines advise including external cause codes to detail the source, location, and intent of the burn. However, payer acceptance may vary.
- External cause codes specify how the burn occurred.
- Agent codes identify the specific substance causing a chemical burn.
Figure 2a: Rule of Nines for Infants
Figure 2b: Rule of Nines for Adults
CPT® Coding for Burn Care: Utilizing the Lund-Browder Chart
CPT® codes for local burn treatment and skin grafting procedures often specify the TBSA treated. CPT® employs the Lund-Browder classification, a more precise method for calculating TBSA for burns and grafts. This method divides the body into 19 regions and uses six age groups to account for body proportion changes from infancy to adulthood. The CPT® code book includes a Lund-Browder chart (See Table 1) for easy TBSA calculation based on body area and age.
Table 1: Lund-Browder Classification Method Chart
| Area | Birth-1 year | 1-4 years | 5-9 years | 10-14 years | 15 year | Adult |
|---|---|---|---|---|---|---|
| Head | 19% | 17% | 13% | 11% | 9% | 7% |
| Neck | 2% | 2% | 2% | 2% | 2% | 2% |
| Anterior trunk | 13% | 13% | 13% | 13% | 13% | 13% |
| Posterior trunk | 13% | 13% | 13% | 13% | 13% | 13% |
| Right buttock | 2.5% | 2.5% | 2.5% | 2.5% | 2.5% | 2.5% |
| Left buttock | 2.5% | 2.5% | 2.5% | 2.5% | 2.5% | 2.5% |
| Genitalia | 1% | 1% | 1% | 1% | 1% | 1% |
| Right upper arm | 4% | 4% | 4% | 4% | 4% | 4% |
| Left upper arm | 4% | 4% | 4% | 4% | 4% | 4% |
| Right lower arm | 3% | 3% | 3% | 3% | 3% | 3% |
| Left lower arm | 3% | 3% | 3% | 3% | 3% | 3% |
| Right hand | 2.5% | 2.5% | 2.5% | 2.5% | 2.5% | 2.5% |
| Left hand | 2.5% | 2.5% | 2.5% | 2.5% | 2.5% | 2.5% |
| Right thigh | 5.5% | 6.5% | 8% | 8.5% | 9% | 9.5% |
| Left thigh | 5.5% | 6.5% | 8% | 8.5% | 9% | 9.5% |
| Right leg | 5% | 5% | 5.5% | 6% | 6.5% | 7% |
| Left leg | 5% | 5% | 5.5% | 6% | 6.5% | 7% |
| Right foot | 3.5% | 3.5% | 3.5% | 3.5% | 3.5% | 3.5% |
| Left foot | 3.5% | 3.5% | 3.5% | 3.5% | 3.5% | 3.5% |
Selecting the correct CPT® code for burn treatment depends on documenting the burn degree and TBSA. Accurate documentation of procedures performed, such as dressing changes or debridement, is essential for coding. Common CPT® codes for burn treatment include:
- 16000: Initial treatment, first-degree burn, when only local treatment is needed.
- 16020: Dressings and/or debridement of partial-thickness burns, initial or subsequent; small (less than 5% TBSA).
- 16025: Dressings and/or debridement of partial-thickness burns, initial or subsequent; medium (e.g., whole face or extremity, or 5% to 10% TBSA).
- 16030: Dressings and/or debridement of partial-thickness burns, initial or subsequent; large (e.g., more than 1 extremity, or greater than 10% TBSA).
Note that code 16000 is exclusively for initial treatment of first-degree burns. Codes 16020, 16025, and 16030 are applicable for initial and subsequent treatments of second- and third-degree burns. Burn treatment codes can be reported with an office visit code if the visit is medically necessary and separately identifiable. In such cases, append modifier 25 to the office visit code. A separate office visit might be necessary to prescribe medications like topical ointments, antibiotics, or pain relievers.
Example Scenario:
Consider a 35-year-old cook who sustained burns from hot cooking oil. He has second-degree burns on the left forearm, first-degree burns on the anterior head, face, and neck, and a third-degree burn on the anterior chest. This is his first visit for burn evaluation. Debridement and dressings are applied to the second- and third-degree burn areas.
ICD-10-CM Coding:
Sequence diagnosis codes by severity:
- T21.31XA Burn of third degree of chest wall, initial encounter (primary diagnosis due to highest severity)
- T22.212A Burn of second degree of left forearm, initial encounter
- T20.19XA Burn of first degree of multiple sites of head, face, and neck, initial encounter
Calculate TBSA using the Rule of Nines: anterior left arm (4.5%), anterior head and neck (4.5%), and anterior trunk (18%) = 27% TBSA.
Extent code: T31.21 Burns involving 20-29% of body surface with 10-19% third degree burns.
External cause codes: X10.2XXA Contact with fats and cooking oils, initial encounter and Y92.511 Restaurant or cafe as the place of occurrence of the external cause.
CPT® Coding:
Using the Lund-Browder chart, estimate the treated burn area at 16%, including the partial-thickness forearm burn (3%) and full-thickness chest burn (13%). The first-degree burns require only local treatment (not separately coded with CPT).
CPT® code: 16030 Dressings and/or debridement of large burn (greater than 10% TBSA).
Conclusion: Mastering Burn Care Coding for Accuracy and Compliance
Accurate burn care coding requires a thorough understanding of burn classifications, ICD-10-CM, and CPT® guidelines. By correctly applying the Rule of Nines or Lund-Browder chart and understanding the nuances of burn degrees and types, medical coders can ensure precise and compliant billing for burn treatments. Proficiency in these guidelines is not only essential for accurate reimbursement but also for reflecting the complexity and severity of burn injuries in patient records.
Resource: American Burn Association, Scald Statistics, and Data Resources
[