
Fracture care coding can be intricate, demanding precision and a thorough understanding of various fracture types, treatment methodologies, and billing protocols. For professionals in automotive-related fields, especially those dealing with accident repairs and insurance claims, a foundational grasp of these coding principles can be invaluable. This article delves into the essentials of fracture care coding, drawing upon the authoritative guidelines from the American Academy of Professional Coders (AAPC) to ensure accuracy and compliance.
Understanding the Basics of Fractures
Contrary to common misconceptions, in medical terms, “fracture” and “broken bone” are synonymous. It’s not just a hairline break; any disruption in the continuity of a bone is classified as a fracture.
Fractures are diverse and categorized based on their pattern and severity. Some common types include:
- Transverse Fractures: A fracture line perpendicular to the bone’s long axis.
- Oblique Fractures: A fracture line that runs diagonally across the bone.
- Spiral Fractures: A fracture line encircling the bone, often caused by twisting injuries.
- Angulated Fractures: Fracture fragments are misaligned at an angle.
- Displaced Fractures: Fracture fragments are separated and not in anatomical alignment.
- Angulated and Displaced Fractures: Combining both misalignment and separation of bone fragments.
Beyond these general categories, numerous specific fracture types are identified by their location, the bone involved, or the mechanism of injury. Examples include:
- Barton’s Fracture: Affecting the distal radius and wrist joint.
- Fissure Fracture: A surface crack in a long bone.
- Jefferson’s Fracture: Fracture of the first cervical vertebra (atlas).
- Lead Pipe Fracture: Compression and slight cracking of the bone cortex.
- Parry Fracture/Monteggia’s Fracture: Ulna fracture with radius head dislocation.
- Ping-Pong Fracture: Depressed skull fracture, typically in children.
- Pott’s Fracture: Fracture of the lower fibula with tibial articulation injury.
- Colles’ Fracture: Distal radius fracture with backward displacement.
Having a medical dictionary or coding resource readily available is crucial when reviewing fracture documentation and encountering unfamiliar terminology.
Fracture Treatment and Reduction: Coding Determinants
The primary goal of fracture treatment is to facilitate proper bone healing, typically achieved through immobilization. This often involves casting or surgical intervention to stabilize the broken bone. Before these procedures, reduction, the process of restoring the fractured bone to its correct alignment, is necessary.
Reduction can be:
- Closed Reduction: Manipulation of the fracture externally, without surgical incision.
- Open Reduction: Surgical exposure of the fracture site to manipulate and realign the bone fragments.
For accurate coding, it’s essential to know the type of reduction performed, the affected body part (arm, leg, finger, etc.), and sometimes the precise fracture location (e.g., femur head vs. shaft).
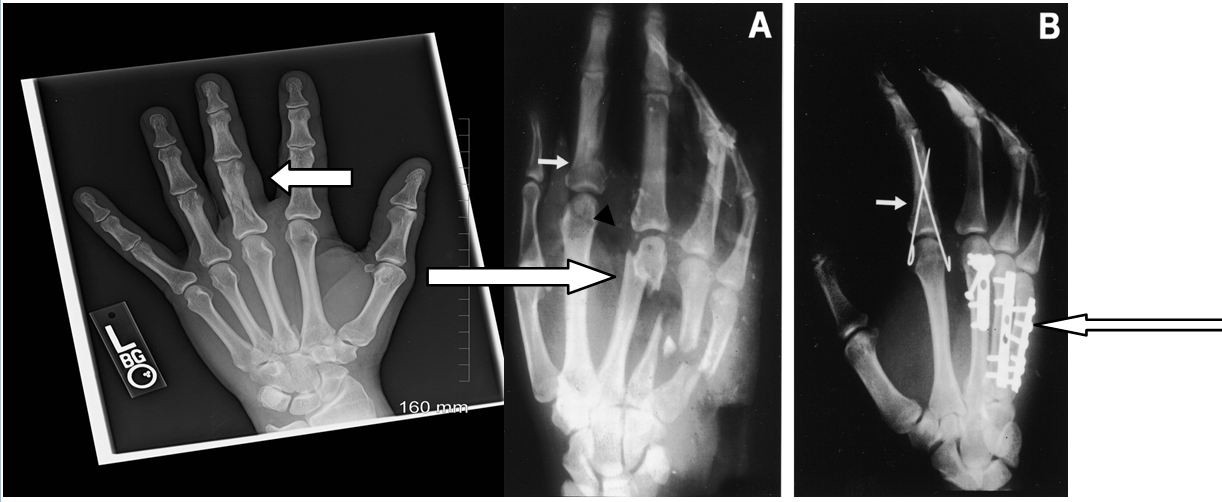
Consider the following X-ray examples illustrating different fracture types and reduction methods:
- Film A (Left): Shows a minimally displaced fracture of the proximal phalanx of the third finger (long finger). This could be coded as closed treatment without manipulation (CPT® 26720) or with manipulation (CPT® 26725), depending on the documented procedure. The short arrow indicates a displaced index finger fracture, while the long arrow points to multiple metacarpal fractures.
- Film B (Right): Demonstrates fracture fixation. The short arrow indicates percutaneous pin fixation (CPT® 26727), and the long arrow shows internal fixation with plates and screws (CPT® 26615). Various internal fixation methods, such as rods and spheres, are also used in fracture care.
Billing for Fracture Care: Global Fees vs. Alternative Methods
According to the American Academy of Orthopaedic Surgeons (AAOS) and the American Medical Association (AMA), two primary approaches exist for coding non-manipulative fracture care services. These are further elaborated in CPT® Assistant publications.
-
Fracture Global Fees: This method, as defined by the AAOS Guide to CPT® Coding for Orthopaedic Surgery, may encompass the initial hospital or office encounter in certain payment contexts. CMS (Centers for Medicare & Medicaid Services) may allow coding an Evaluation and Management (E/M) service with modifier -57 (Decision for surgery) if the initial visit was when the decision for surgery was made. The global fee typically covers the initial cast or splint application and all follow-up visits within a 90-day period from the initial fracture treatment, excluding physician-obtained radiographs. Recasting or re-splinting are usually billed separately per encounter.
-
Alternative Method for Fracture Fees: This approach applies when fracture treatment doesn’t primarily involve a “procedure,” such as closed treatment without manipulation. Services are itemized as if it were a standard office encounter. Examples include undisplaced fifth metatarsal fractures, minimally displaced pelvic fractures, or vertebral compression fractures. Office, hospital, and emergency department encounters are coded accordingly, along with injections, supplies, casts, splints, or other necessary treatment components.
It’s crucial to note that payer-specific guidelines prevail. When fracture care is provided in an office setting, some payers may require modifier 25 (Significant, separately identifiable evaluation and management service by the same physician on the same day of the procedure or other service) to be appended to the E/M service code. Practices must determine whether to bill globally or itemize based on specific circumstances and payer requirements.
Coding Examples: Applying Fracture Care Billing Methods
Coding Example No. 1: Closed Reduction without Manipulation vs. E/M
Consider the coding implications of choosing between reporting closed reduction without manipulation versus an E/M service.
Reporting Closed Reduction w/o Manipulation:
- Cast/splint/strapping is included in the procedure code.
- X-rays and supplies can be reported separately.
Reporting an E/M Service:
- Cast/splint application, X-rays, and supplies can all be reported separately, in addition to the E/M code.
Closed reduction codes encompass a 90-day global package. The initial casting, splinting, and strapping, along with routine postoperative visits, are included. However, X-rays, DME, and casting/splinting supplies are billed separately. Within the global period, separate charges for related E/M services are not permissible. For instance, for a closed reduction with manipulation (CPT® 26725):
- Procedure: 26725
- Do not code separately for cast or splint application.
- Next visit (if required and related to the procedure within the global period): 99024 (Postoperative follow-up visit, included in surgical package)
- No separate E/M coding is allowed for related services during the 90-day global period.
- Casting and/or splinting supply charges can be reported based on documentation.
Coding Example No. 2: Undisplaced Clavicle Fracture and Initial Sling Application
A patient presents with an undisplaced clavicle fracture, is provided a sling, and instructed to follow up as needed (PRN). Can fracture care coding be applied? Is this considered complete treatment if no scheduled follow-up is planned?
Remember that fracture care codes, like surgical procedures, have preoperative, operative, and postoperative components reflected in physician reimbursement:
- 17% Preoperative
- 63% Operative
- 20% Postoperative
In this scenario, if there is no intention for the provider to offer follow-up care, the postoperative component is absent. Billing a fracture treatment code might be inappropriate. Similar to an ED physician treating a fracture without follow-up, reporting an appropriate E/M service code would be more accurate than a fracture care code.
Coding Example No. 3: Fracture Care Split Between Providers in Different Locations
A patient injured in Utah undergoes surgery and returns home to New Jersey for follow-up care. How is reimbursement handled?
Ideally, the Utah surgeon should receive 17% (preoperative) + 63% (operative) of the reimbursement. If aware of the patient’s out-of-state follow-up, they should append modifier 54 (Surgical care only) to the fracture care code and inform the New Jersey orthopedist of the transfer of care in writing. The New Jersey orthopedist, accepting postoperative care, should bill the same surgical code with modifier 55 (Postoperative care) to receive the 20% postoperative fee.
However, in practice, such ideal splits are rare. Often, the initial surgeon may be reluctant to relinquish the postoperative portion of the fee. In such cases, communication is key. The orthopedist providing follow-up care should contact the initial surgeon to discuss a fee split. If agreed upon and the initial claim is already filed, a corrected claim is necessary. Without communication and documented transfer of care, billing for postoperative care is not permissible.
Essential Tools for Orthopaedic Coding
For those involved in orthopaedic coding, continuous learning and access to up-to-date resources are vital. AAPC offers valuable tools and certifications to enhance expertise and ensure coding accuracy. Consider pursuing the Certified Orthopaedic Surgery Coder (COSC™) certification to demonstrate proficiency in this specialized area. Utilizing current medical coding books and resources like AAPC Coder for efficient code searches are also highly recommended for navigating the complexities of fracture care and other orthopaedic coding scenarios.
Author Bio: Cynthia Everlith, BSHA, CPC, CMA, is practice administrator for Arizona Hand and Wrist Specialists, a division of OSNA, PLLC. She has more than 25 years of experience in orthopaedic coding and practice management, and 16 years with her current practice. She is actively involved in workers’ compensation legislation and has worked closely with the Industrial Commission of Arizona and the Arizona Medical Association in rules affecting physicians. She has presented nationally and locally. She is a past American Association of Orthopaedic Executives (AAOE) Board of Directors and past president of AAPC’s Grand Canyon Coders Phoenix chapter. She serves on the AAOE Communication Council and Technology Task Force, and is president of the Arizona AAOE Chapter.